Last Updated on March 5, 2025 5:51 pm by INDIAN AWAAZ
Cushing syndrome happens when the body has too much of the hormone cortisol for a long time. This can result from the body making too much cortisol, or from taking medicines called glucocorticoids, which affect the body the same way as cortisol.
Dr Nitin Kapoor and Dr Sanjay Kalra
Selective screening of persons with metabolically unhealthy obesity for Cushings syndrome is more likely to increase the probability of diagnosing Cushing syndrome, suggests a study from Turkey published Aug. 9, 2024, in the International Journal of Obesity.1
A team of endocrinologists from Turkey retrospectively analyzed data from 1008 patients with obesity who underwent screening for Cushing’s syndrome at an endocrinology outpatient clinic between December 2020 and June 2022. Their mean age was 40 years, and the majority were female (~83%). The median BMI was 43.7 kg/m². Based on the presence of comorbid conditions, 779 were categorized as metabolically unhealthy obesity (MUO); 23% had diabetes, 29% had prediabetes, ~25% had hypertension and 78% had dyslipidemia; less than 5% had coronary artery disease. The remaining 229 had metabolically healthy obesity (MHO). The 1mg overnight dexamethasone-suppression test (DST) was utilized to screen for Cushing’s syndrome. A serum cortisol level < 1.8 µg/dL indicated normal suppression.
The cortisol levels following the 1 mg DST were significantly higher in those with metabolically unhealthy obesity vis a vis metabolically healthy obesity. About 1.2% (n=12) patients within the entire study group had a cortisol level of ≥ 1.8 following the 1 mg DST. Eleven of the 12 patients with a cortisol level of ≥ 1.8 had MUO. This group also had higher fasting plasma glucose, HbA1c, triglyceride, and LDL cholesterol levels and lower HDL cholesterol levels. Hypercortisolism was definitively diagnosed in two patients with an ensuing overall prevalence of 0.2%. The specificity of the 1 mg DST in screening for Cushing’s syndrome was 99%, while the sensitivity was 100%.
This study highlights two main findings. Firstly, it demonstrates the high specificity of the 1 mg DST as a screening test for Cushings syndrome, including in patients with obesity. This has clinical relevance since there is considerable overlap of signs and symptoms between the two conditions. Secondly, it reaffirms the low prevalence of Cushing’s syndrome in patients with obesity, which per se is a rare condition. Hence, rather than screening all individuals with obesity, it would be more prudent to screen those with the metabolically unhealthy obesity (MUO) phenotype.
Reference
1. Sema Hepsen, et al. Cushings syndrome screening with the 1-mg dexamethasone suppression test in metabolically healthy and unhealthy obesity phenotypes. Int J Obes (Lond). 2024 Aug 9. doi: 10.1038/s41366-024-01598-0.
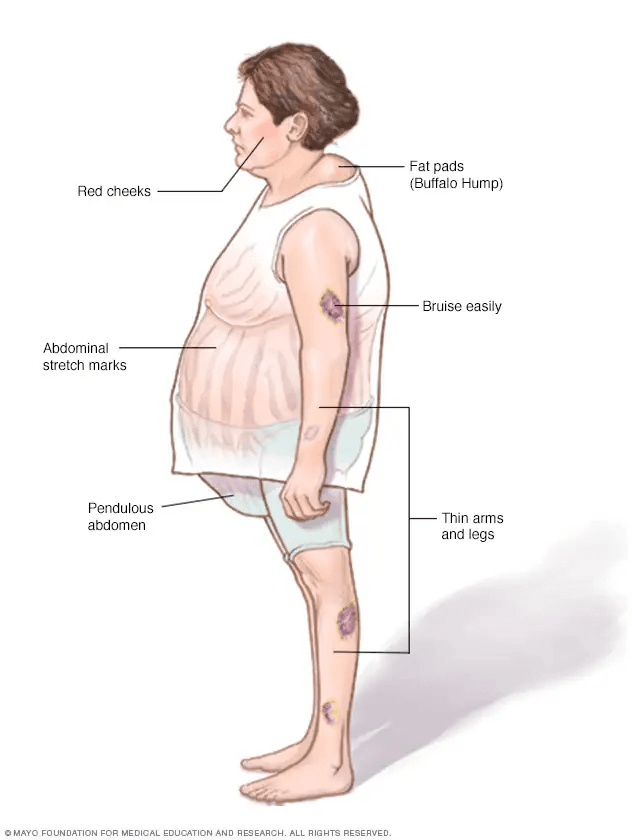
Common symptoms of Cushing syndrome
- Weight gain in the trunk, with thin arms and legs.
- Weight gain in the face. This is sometimes called moon face.
- A fatty lump between the shoulders. This may be referred to as a buffalo hump.
- Pink or purple stretch marks on the stomach, hips, thighs, breasts and underarms.
- Thin, frail skin that bruises easily.
- Slow wound healing.
- Acne.
Symptoms women with Cushing syndrome may experience
- Thick, dark hair on the face and body. This condition is called hirsutism.
- Periods that are irregular or that stop.
Symptoms men with Cushing syndrome may experience
- Lower sex drive.
- Reduced fertility.
- Problems getting an erection.
Other possible symptoms of Cushing syndrome
- Extreme tiredness.
- Muscle weakness.
- Depression, anxiety and irritability.
- Emotions that are hard to control.
- Trouble concentrating or remembering.
- Sleeplessness.
- High blood pressure.
- Headache.
- Infections.
- Skin darkening.
- Bone loss, which can lead to broken bones.
- Stunted growth in children.